Bone is a living, growing tissue that is constantly rebuilding itself, replacing old weak bone with new fresh bone. To do this your body breaks down and dissolves old bone into minerals and collagen and then recycles these products into the growing new bone.
In order to keep bones healthy, it is important tmatrihat the amount of bone that is removed is replaced with the same amount of new bone. This is called remodelling.
Throughout your lifetime, your bones are constantly being remodelled to maintain a healthy bone structure. Bone turns over at a rate of about 10 per cent a year. This constant remodelling keeps your bones strong, as it repairs the microscopic cracks that are made as part of daily activity. Bone remodelling takes place all the time throughout your body.
In young, healthy people, the amount of bone formed is usually more than the amount removed but as we age, more bone is removed than formed causing a gradual loss of bone structure and strength. This can lead to the bone disorder known as osteoporosis (which means porous bones).
Bone turnover markers are substances that are made as bones remodel themselves as part of the natural regeneration cycle. They can be found in your blood and urine.
How does bone rebuild itself?
Bone begins as a flexible scaffold made by special cells which lay down type-1 collagen, a tough fibrous type of protein that acts as a framework. Next, minerals which circulate in the bloodstream, calcium and phosphate start to crystalise within the framework. This gives the bone its structure and strength.
There are two main types of cells involved in maintaining bone: osteoclasts and osteoblasts.
What causes bone loss?
During early childhood and in the teenage years, new bone is added faster than old bone is removed. People generally reach their peak bone density and strength between the ages of 25 and 30. The age at which someone starts to see some bone loss depends on the amount of bone that was developed during their youth and the rate of bone resorption.
After this peak period, bone loss occurs faster than the rate of bone formation, leading to bone loss. Women, who generally have smaller, lighter bones than men, experience bone loss earlier than men and after menopause the rate of bone loss speeds up due to a drop in oestrogen levels.
Each remodelling cycle leaves the bone a little thinner than before. Anything that speeds up the breakdown of bones or slows down the rebuilding process raises your risk of having osteoporosis.
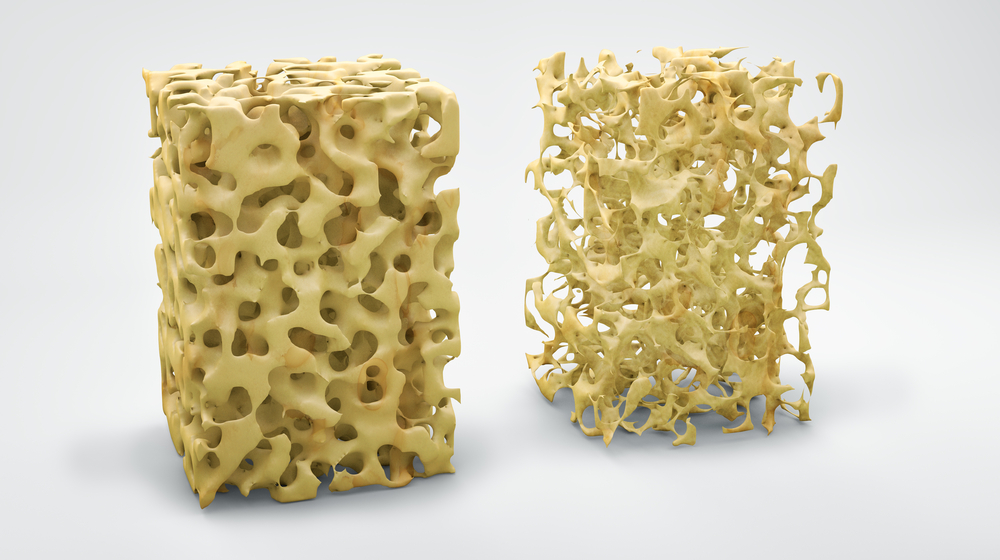
In osteoporosis, your bones lose too much density and become fragile, making them more likely to break. The spongy inner mesh develops larger gaps and thinner struts, making it less able to absorb force. The hard outer shell of bone becomes thinner and more porous.
As well as ageing, several diseases and conditions can cause bone loss. These include:

Diagnosing bone loss
If you are being investigated for bone loss you will have a bone density scan, also known as a DEXA scan which measures the density of bones in the spine and hip. If the scan detects bone loss and/or if you have a history of unexpected bone fracture, a range of blood and urine tests will be needed.
| Blood tests | Why they are done |
You need calcium and phosphate to give your bone the structure and hardness it needs. There are two main types of calcium in your blood. One circulates in your blood and is called free or ionised calcium, and the other is bound to albumin, the main protein in your blood. You have roughly equal amounts of free calcium circulating in your blood and bound calcium attached to proteins. Both are tested. | |
| Albumin | If you have a low albumin level, your total calcium might appear low even if the active, ionised calcium levels are normal. Conversely, high albumin can make total calcium look falsely high. Measuring albumin helps estimate your calcium status more accurately. |
| Creatinine and GGT | These tests assess kidney and liver function, which influence bone metabolism. |
| Parathyroid Hormone (PTH) | Your body works to keep calcium at just the right balance. Levels are kept in balance through a feedback system under the control of your parathyroid glands, which are tiny glands at the back of your thyroid. |
| Vitamin D | Vitamin D helps your body absorb calcium and phosphate from your diet. |
| Alkaline Phosphatase (ALP) | ALP is used in bone mineralisation and levels can reflect the rate of bone formation. |
| Urine tests | |
| Urine Calcium | This shows how much calcium is being lost in your urine. |
| Urine Phosphate | This can show if you are losing too much phosphate through your kidneys or are not absorbing enough from your diet. |
| Urine Creatinine | This is used to help in interpreting other urine tests. |
| For more information, please click on each of the tests. | |
Bone turnover markers
Bone turnover markers are substances measured in blood or urine that show how actively your bone is being formed and broken down. They help understand how fast bone tissue is turning over.
| Bone formation markers (new bone is actively being made) | |
| P1NP (Procollagen type 1 N propeptide) | P1NP is a protein released when new bone is formed. |
| Bone resorption markers (bone is being broken down) | |
| CTx (C-terminal telopeptide) | CTx is a substance released when bone breaks down |
| Urine tests that are sometimes used | |
| NTx (N-terminal telopeptide) urine test | NTx is a substance released during bone resorption |
| DPD (Deoxypyridinoline) urine test | DPD is a substance released during bone resorption |
Sample
Bone markers can be measured in blood, urine, or both, depending on which markers are being tested and why.
Any preparation?
Fasting may be required before testing and samples are typically collected in the morning. Many bone markers in the blood and urine vary in concentrations depending on the time of day (diurnal variation), so sample timing can be important. Carefully follow any instructions given for the timing of blood and urine sample collections, especially if you are having a Fasting Bone Metabolic Study.
Reading your test report
Your results will be presented along with those of your other tests on the same form. You will see separate columns or lines for each of these tests.
Reference intervals - comparing your results to the healthy population
Your results will be compared to reference intervals (sometimes called a normal range).
If your results are flagged as high or low this does not necessarily mean that anything is wrong. It depends on your personal situation.
Reference intervals for bone turnover markers vary between labs so you will need to go through your results with your doctor.
Fracture risk assessment
Bone turnover markers are currently not recommended for fracture risk assessment and therefore not included in fracture risk calculators. However, they are valuable tools for monitoring, particularly for people with osteoporosis.
Bone turnover markers are used to provide further information. They are most useful when used in conjunction with other established risk assessment tools, such as the FRAX® or Garvan calculators and BMD (bone mineral density) measurements.
High levels of bone turnover markers, such as CTx, can indicate a higher fracture risk, especially if you have a low BMD. The highest risk is seen in people with both low BMD and high bone turnover. Bone turnover markers cannot show the cause of the problem.
Important considerations
Caution is needed in interpreting test results as they can be affected by diet, exercise, and the time of day the sample is collected.
Your results need to be interpreted by your doctor. Usually, you will be having these tests when seeing a specialist doctor. Concentrations of bone markers are affected by many factors, particularly during childhood development. These include age, sex, growth velocity, nutritional status and puberty. Other clinical risk factors, such as age, history of fractures and medication use (such as glucocorticoids), should always be considered alongside BMD and bone turnover marker levels.
Very high bone turnover marker levels can be a sign of conditions other than postmenopausal osteoporosis, such as hyperparathyroidism, hyperthyroidism, Paget's disease or malignancy (cancer).
The choice of tests your doctor makes will be based on your medical history and symptoms. It is important that you tell them everything you think might help.
You play a central role in making sure your test results are accurate. Do everything you can to make sure the information you provide is correct and follow instructions closely.
Talk to your doctor about any medications you are taking. Find out if you need to fast or stop any particular foods or supplements. These may affect your results. Ask:
Pathology and diagnostic imaging reports can be added to your My Health Record. You and your healthcare provider can now access your results whenever and wherever needed.
Get further trustworthy health information and advice from healthdirect.